A Tibial Plateau Levelling Osteotomy (TPLO) is one of the most common surgeries I see in Physiotherapy clinic, so if your dog is due to have or has had a TPLO please do not panic! This blog is targeted at owners so you can learn about why a TPLO is needed and the role of Physiotherapy. I strongly feel owners need to feel educated and informed about their dog’s next steps so the right decisions can be made. So, let’s start from the beginning!
Why would my dog need a TPLO?
A TPLO is a type of surgery used to treat either a partial or fully ruptured Cranial Cruciate Ligament (CCL). When thinking about this in humans, a CCL is the same as an Anterior Cruciate Ligament (ACL) which works exactly the same. The CCL (or ACL) helps to stabilise the knee by preventing forward movement of the tibia on the femur (the shin bone and the thigh bone).
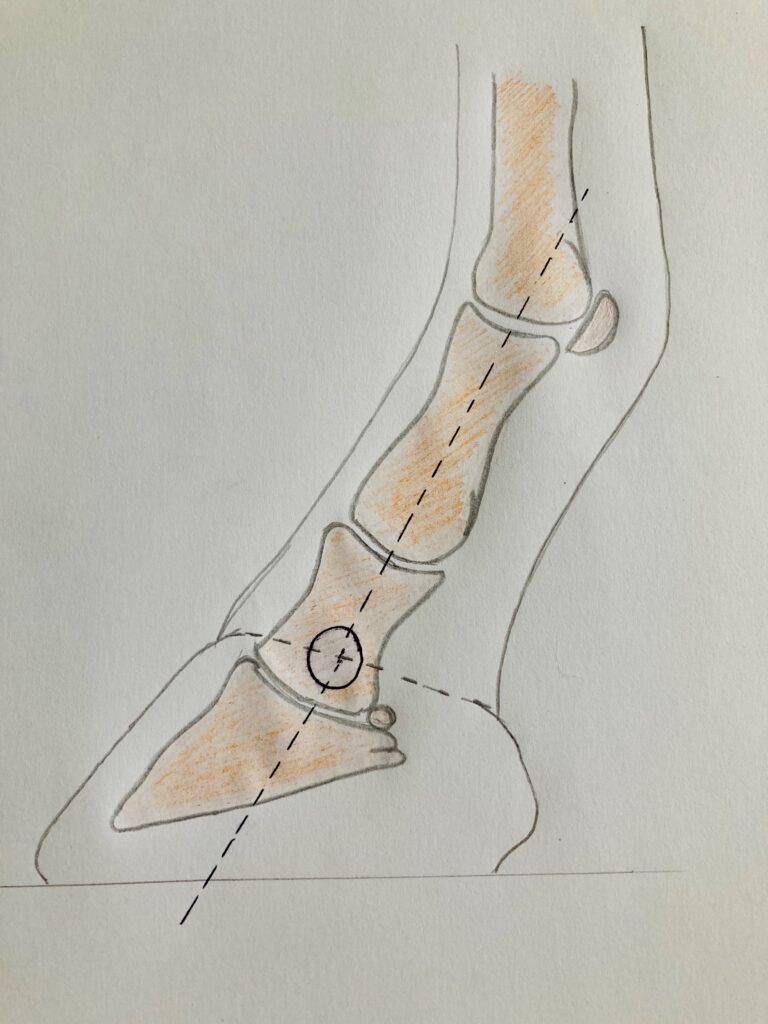
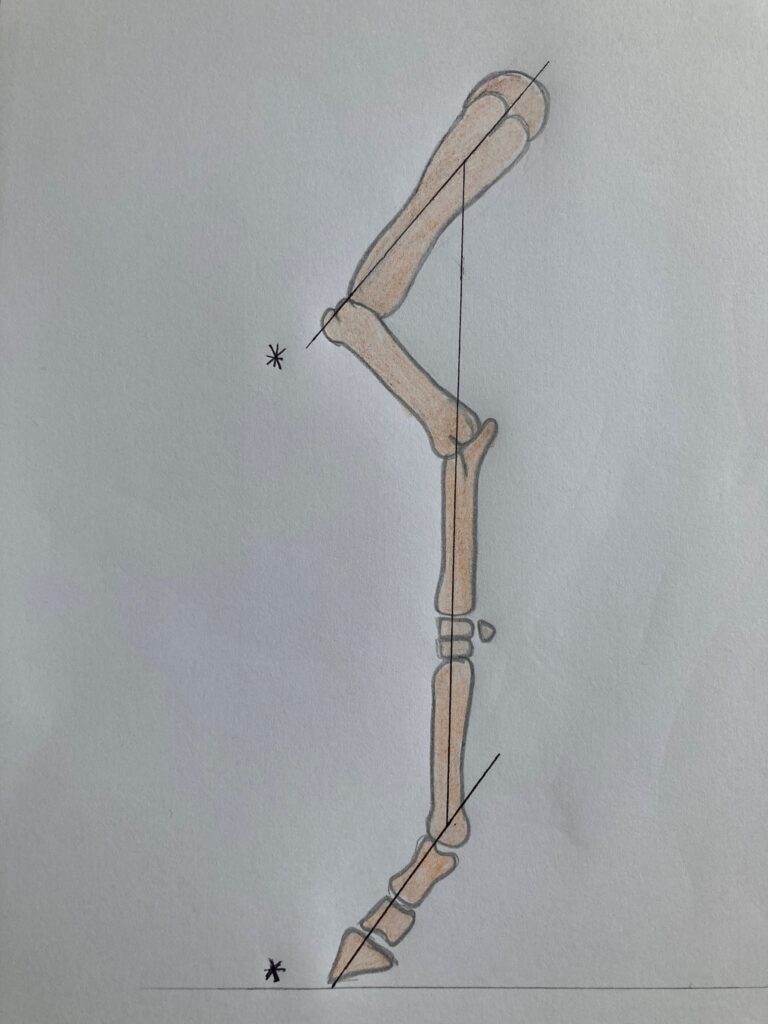
When you read about the cause of a CCL rupture you will see the term ‘degenerative changes’. Now I tend to dislike that phrase and something I refrain from using in my human practice, mainly because the wording can have negative or worrying connotations for patients. It sounds so much worse than what it means. I tend to use the analogy, ‘it’s like when your hair goes grey’ because it’s a ‘natural ageing process within the body’, so overtime the ligament can weaken. This process can also be accelerated by other factors, such as weight, breed, or conformation so in some cases dogs can be quite young and have this injury. Another added cause to a CCL injury is how the dog is anatomically made. In standing a dog will stand with roughly 110degrees of knee bend (on average), which means the CCL is always under strain. When there is strain or tension, intrinsic stress can occur in the joint and the risk of injury is higher, hence why younger dogs can sustain this injury.

What are the symptoms of a CCL rupture?
The symptoms overall are obvious to owners because your dog just won’t be their normal self. I have written the most obvious symptoms below.
- Inability to put their full weight through the leg – pain and inflammation are common drivers to this because of the excessive movement of the tibia on the femur.
- Stiffness on rising, getting out of bed, after walks or at the start and end of the day – this is usually due to the level of swelling within the joint but also the muscles around the joint becoming inactive and tight.
- Aggression to other dogs or sometimes people due to the level of pain.
- Reluctance to go upstairs, jump in and out of the car or the sofa.
What is a TPLO?
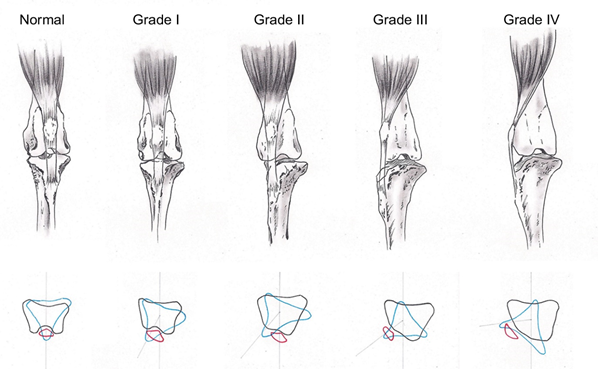
A TPLO is one type of surgery used for this injury, it is widely performed and first described in 1993. It involves cutting into the bone called the tibial plateau (top of the tibia) and rotating it, meaning the tibia cannot slide anymore. It ultimately stabilises the knee immediately and reduces the risk of further complications, such as osteoarthritis. A plate is then put in place to secure the rotated bone and promote healing. Despite the surgery sounding quite intense it is very routine. There are some useful images here https://www.ndsr.co.uk/specialist-referral-service/pet-health-information/orthopaedic-surgery/tplo-surgery.
So where does Physiotherapy come in?
A human would have Physiotherapy after an ACL injury and so should your dog.
There are various things Physiotherapy can do after a TPLO with the focus of reducing pain, promoting tissue healing and reducing compensatory strategies. When these three aspects align, flexibility, strength, balance, and confidence will return, and your dog will be back to their usual tricks again within no time. Some patients require weekly sessions after a TPLO, whereas others need more of an observational approach and this is because every dog is different and every rehabilitation journey is different, so it must be tailored to you and your dog’s needs!
An assessment will always be conducted first where the physiotherapist will assess your dog’s gait, the wound, range of motion, muscle bulk, motor control, posture, and neurology. One other large aspect of physiotherapy is to prevent the risk of injury in other areas whilst they are recovering, for example after a TPLO the dog will naturally offload the limb and quite cleverly move their centre of mass forward. The risk of forelimb and shoulder pathologies can increase if this posture is maintained so this is usually targeted early in the rehabilitation programme.
As time and healing progresses so does the Physiotherapy. This might include the introduction of a strengthening programme starting from static and ranging from plyometrics and fitness rehabilitation. Everything is tailored to your dog and their lifestyle.
I hope this has been beneficial and if I had more time I could keep writing and talking, so if you have any questions please do contact us, even if its just to say hello!
See you soon!!